Breathing (hereinafter — “D.”; this article is in russian — Дыхание) — is a set of processes that provide the flow of oxygen into the body and the release of carbon dioxide (external D.) and the use of oxygen by cells and tissues for the oxidation of organic substances with the release of the energy contained in them, necessary for life (tissue respiration, cellular D.). Oxygen-free way of energy release is peculiar only to a small group of organisms-the so-called anaerobes; during the evolution of the release of energy as a result of D. the vast majority of organisms became the main process, and anaerobic reactions remained mainly as intermediate stages of metabolism.
The breath of animals and humans
In protozoa, sponges, coelenterates and some other organisms O2 diffuses directly through the surface of the body. With the complication of the organization and increase in body size there are special breathing organs, as well as the circulatory system, which circulates the liquid — blood or hemolymph containing substances that can bind and carry O2 and CO2 (see hemoglobin). In insects, O2 enters the tissues from the system of air — borne tubes-trachea. In aquatic animals, using dissolved in water O2, respiratory gills are provided with a rich network of blood vessels. In this case, O2 dissolved in water diffuses into the blood circulating in the vessels of Gill slits. In many fish, the intestinal D. plays a significant role, in which air is swallowed and O2 enters the blood through the blood vessels of the intestine; some role In D. fish also plays a swimming bubble; many animals living in the water exchange of gases (mainly CO2) occurs through the skin.
In land animals external respiration is provided mainly by lungs. In amphibians and many other animals along with this functioning of the skin. D. the birds were essential in communicating with light air bags that change the amount of aircraft movements and facilitate D. in flight. In amphibians and reptiles, air is pumped into the lungs by the movements of the muscles of the mouth bottom. In birds, mammals and humans, the external D. is provided by the rhythmic work of the respiratory muscles (mainly the diaphragm and intercostal muscles), coordinated by the nervous system. With the reduction of these muscles, the volume of the chest increases and stretching of the lungs in it occurs; therefore, there is a difference between atmospheric and intra-pulmonary pressure and air enters the lungs (breath). The exhalation can be passive-due to the decline of the chest stretched during inhalation, and after it and the lungs; active exhalation is due to the reduction of some muscle groups. The amount of air entering the lungs after 1 breath is called the respiratory volume.
When breathing, the respiratory musculature overcomes the elastic resistance associated with the elasticity of the chest, lung traction and surface tension of the alveoli. The latter, however, is significantly reduced under the influence of the surfactant produced by the cells of the alveolar epithelium; therefore, the alveoli do not fall down during exhalation, and easily expand during inhalation. The higher the elastic resistance, the more difficult to stretch the chest and lungs; with deep D. the work of the respiratory muscles, spent on overcoming it, increases dramatically. Non-elastic resistance D. it is mainly due to the friction of the air when it moves along the nasal passages, larynx, trachea and bronchi. It depends on the speed of air flow during on and his character. With quiet breathing, the flow is close to laminar (linear) in straight sections of the Airways and to turbulent (vortex) in places of branching or contraction. With increasing flow rate (with forced D.) turbulence increases and to promote air requires a higher pressure difference, and hence the increase in the work of the respiratory muscles. The uneven distribution of resistance to air movement along the respiratory tract leads to the fact that the air flow to different groups of pulmonary alveoli occurs unevenly; this difference in ventilation is especially significant in pulmonary diseases.

The amount of air ventilating the lungs in 1 minute is called minute volume of respiration (MOD). MOD is the product of the respiratory volume at a frequency D. (the number of respiratory movements in 1 min, equal to a person about 15-18) and is an adult at rest 5-8 l/min. Only part of the MOD (about 70%) involved in the exchange of gases between the inhaled and alveolar air, this part is called the volume of alveolar ventilation; the rest of the MOD is used to” flush ” the so-called dead, or harmful, airway space, in which by the beginning of the exhalation the outside air is stored, filling it at the end of the previous inhalation (the volume of the dead space is about 160 ml). Ventilation of the alveoli ensures the constancy of the composition of the alveolar air. The partial pressure of O2 (pО2) and CO2 (pCО2) in alveolar air varies within a very narrow range and is about 13 kN/m2 (100 mm Hg) for O2. St.) and for CO2 of about 5.4 kN/m2 (40 mm Hg. V.).
The exchange of gases between alveolar air and venous blood entering the capillaries of the lungs is carried out through the alveolar-capillary membrane, the total surface of which is very large (in humans about 90 m2). Diffusion of O2 in the blood is provided by the difference of partial pressures of O2 in the alveolar air and in the venous blood (8-9 kN m2, or 60 — 70 mm Hg. V.). CO2 carried in the blood from the tissues in bound form (bicarbonate, salts of carbonic acid and carbenecillin), is released in the capillaries of the lung involving the enzyme carbonic anhydrase diffuses from the blood into the alveoli; the difference of pCО2 between venous blood and alveolar air is about 7 mm Hg. V.
The ability of the alveolar wall to pass O2 and CO2, the so-called diffusion ability of the lungs, is very high: at rest it is in 1 min about 30 ml O2 per 1 mm difference of pО2 between the alveolar air and blood; for CO2 this value is many times greater. Therefore, the partial pressure of gases in the arterial blood flowing from the lungs has time to get closer to their pressure in the alveolar air. The transition of O2 into tissues and removal of CO2 from them also occurs by diffusion, since pО2 in the tissue fluid 2,7 — 5,4 kN/m2 (20 — 40 mm Hg. art.), and in the cells below, and rcO2 in cells can reach 60 mm Hg. St.:
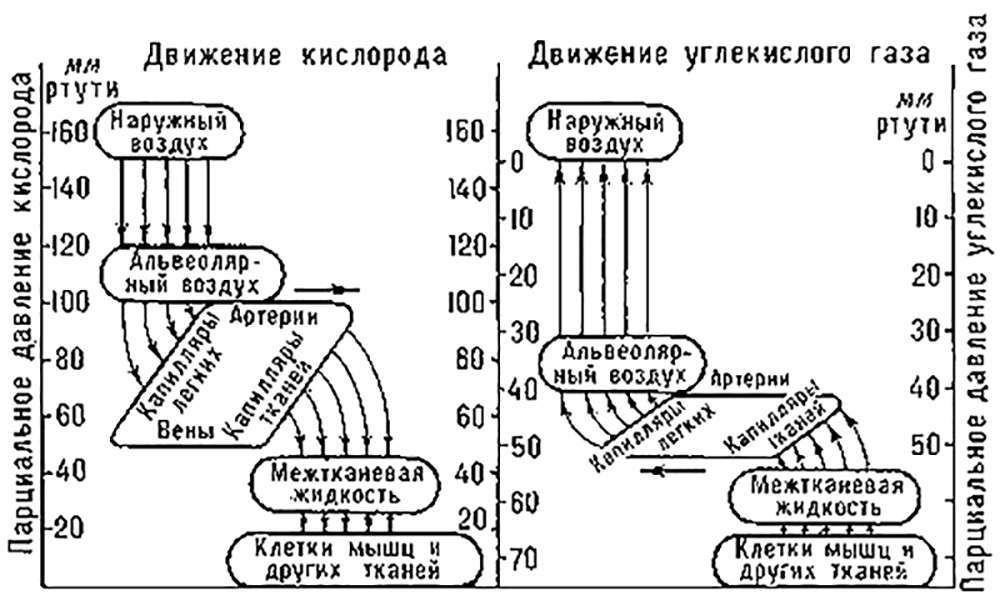
Figure: diagram of the movement of oxygen and carbon dioxide during respiration (click on the picture to enlarge)
The consumption of O2 by cells and tissues and their formation of CO2, which is the essence of tissue, or cellular, respiration, is one of the main forms of dissimilation, which is carried out in animals and plants in principle the same. High O2 consumption characteristic of the tissues of the kidneys, the bark of the big hemispheres of the brain, heart[ru]. As a result of oxidation-reduction reactions of tissue D. released energy spent on all life manifestations. This process is carried out in the mitochondria and consists of dehydrogenation of substrates D. – carbohydrates and products of their breakdown, fats and fatty acids, amino acids and their deamination products. D. substrates absorb O2 and serve as a source of CO2.
Ratio: CO2/O2 is called the respiratory coefficient.
The energy released during the oxidation of organic substances is not used by tissues directly, since about 70% of it is spent on the formation of ATP-one of the adenosine phosphoric acids, the subsequent enzymatic splitting of which provides the energy needs of tissues, organs and the body as a whole (see oxidation biological, oxidative phosphorylation). Thus, from the biochemical point of view, breathing is the transformation of the energy of carbohydrates and other substances into the energy of macroergic phosphate bonds.
The constancy of pО2 and pCO2 in alveolar air, and hence in arterial blood, can be maintained only if alveolar ventilation corresponds to the rate of consumption of O2 and the formation of CO2, i.e. the level of metabolism. This condition is provided by the perfect mechanisms of regulation D. the frequency and depth D. control is carried out by reflex. Thus, increase in pCО2 and decrease in pО2 in the alveolar air and in arterial blood excites the chemoreceptors and kardiotoniki sinocarotid zones, which leads to stimulation of the respiratory centre and increase MOD. According to classical ideas, the increase in rcO2 in the arterial blood, washing the respiratory center, also excites him and causes an increase in MODES. Thus, the regulation Of D. on the deviation of pО2 and CO2 in the arterial blood, carried out by the type of feedback, provides an optimal MODE. However, in some cases, such as muscle work, MOD increases before the onset of metabolic changes that lead to changes in the gas composition of the blood. This increase in ventilation is due to signals coming to the respiratory center from the receptors of the motor apparatus, the motor area of the cerebral cortex, as well as conditional reflexes to various signals associated with the usual work and its environment. Thus, the control of D. is a complex self-learning system not only on the principle of regulation of deviation, but also on the signals warning of possible deviations.
The change of inhalation and exhalation is provided by a system of complementary mechanisms. During exhalation, the respiratory center receives impulses from the stretching receptors located in the lungs through the fibers of the vagus nerves. When the lungs reach a certain volume, this impulse inhibits the cells of the respiratory center, the excitation of which causes inhalation. When you turn off the nerve pathways, providing the arrival of impulses in the respiratory center, the rhythm of breathing is preserved due to the automatism of the center, but the nature of the rhythm is very different from the normal. In violation of D. and the mechanisms of its regulation there are changes in the gas composition of the blood (hypoxia).
Methods of research of breathing are various. In the physiology of work and sports, clinical medicine is widely used registration of the depth and frequency of respiratory movements, measurement of the gas composition of exhaled air, arterial blood, pleural and alveolar pressure. (L. L. Chic)
See also the article: – gas Exchange.
Read more about breathing in the literature:
- Sechenov I. M., Selected works, Moscow, 1935;
- Holden John. and J. Priestley., Breathing, translation from English, M.-L., 1937;
- Marshak M. E., regulation of breathing in humans, M., 1961;
- Human physiology, M., 1966;
- Comroe J. Н., Physiology of respiration, Chi., 1966;
- Dejours P., Respiration, Oxf., 1966.









